|
Hydroxylapatite and Tricalcium Phosphate Implants in the Dental Alveolus of Rats. A Histometric Study
Adalberto Luiz ROSA[1]
Luiz Guilherme BRENTEGANI[2]
Sylvestre Arnaldo GRANDINI[1]
[1]Departamento de Cirurgia,
[2]Departamento de Estomatologia, Faculdade de Odontologia de
Ribeirão Preto, USP, Ribeirão Preto, SP, Brasil
Braz Dent J (1995) 6(2): 103-109 ISSN 0103-6440
| Introduction | Material/Methods
| Results | Discussion
| References |
The objective of the present study was to analyze histomorphometrically
the biological behavior of microgranular hydroxylapatite (MIC), particulate
hydroxylapatite (HA 40), and tricalcium phosphate (TCP) implanted in the
dental alveolus of rats. All three materials retarded alveolar repair when
compared to controls, since less bone was formed during all periods of
study. Nevertheless, MIC and TCP showed higher compatibility than HA 40.
Key words:hydroxylapatite, tricalcium phosphate, alveolar repair.
Introduction
Calcium and phosphate ceramics have been widely used as substitutes for
bone tissue, mainly because they have a composition similar to that of
bone. Among these ceramics, the most frequently used ones are those with
a Ca:P proportion of approximately 1.67 or 1.50, i.e., hydroxylapatite
and tricalcium phosphate.
Clinical evaluations of these ceramics used to coat metal implants,
in the treatment of periodontal lesions, in the prevention of alveolar
ridge resorption and in the recovery of an atrophic alveolar ridge have
shown conflicting results (Block and Kent, 1986; De Wijs et al., 1993).
These facts indicate the need to carry out thorough experimental and
clinical investigations of new ceramics composed of hydroxylapatites or
tricalcium phosphate, in order to determine which materials may be used
in patients and in which clinical situations.
The objective of the present study was to evaluate histometrically the
biological behavior of three calcium and phosphate ceramics differing in
composition and/or in particle size, implanted into the dental alveoli
of rats.
Material and Methods
A total of 80 male rats (Rattus norvegicus, Wistar strain) weighing 120
150 g were submitted to extraction of the right upper incisor. The animals
were divided into 4 groups: control, no treatment; implanted with tricalcium
phosphate (TCP) (S.R. Graft Center Implant, USA) whose granules ranged
in size from 800 to 1200 µm; implanted with microgranular hydroxylapatite
(MIC) (Biohapatita Odontec, São Paulo) whose granules ranged in
size from 10 to 50 µm; implanted with particulate hydroxylapatite
(HA 40) (H.A. 40 Homus, São Paulo) whose granules ranged in size
from 1000 to 2000 µm.
During the experiment the animals were fed a solid diet for rodents
and received water ad libitum, except during the first 24 h after extraction.
The animals were anesthetized intraperitoneally with 40 mg/kg thionembutal
(Abbott, São Paulo). The right upper incisor was then extracted,
irrigated with saline, filled with the materials and sutured with monofilament
nylon. The animals received a bolus dose of Pentabiótico Veterinário
(Fontoura Wyeth, São Bernardo do Campo, SP) intramuscularly.
Five rats were decapitated after each post extraction period, i.e.,
1, 2, 3 and 6 weeks. Their mandibles were separated from the maxillae and
the right maxilla was then separated from the left one with a lancet through
a median sagittal incision along the intermaxillary suture. The specimen
with the right dental alveolus was obtained by a straight scissors cut
tangentially to the distal surface of the molars.
The specimens were immersed in 10% formalin and fixed for 24 h, decalcified,
dehydrated, cleared, embedded in paraffin and oriented so as to permit
6-µm thick longitudinal sections which were stained with hematoxylin
eosin. A total of 20 sections were obtained per block, each section separated
from the other by an interval of 10 sections.
In order to permit a better comparison of the results, in the present
study the middle third of the alveolus was chosen for quantitative analysis.
The histological sections were examined with a binocular light microscope
(Jenamed, Zeiss Jena, Germany) fitted with an immersion objective (100X)
and equipped with a light camera. In each alveolus 10 microscopic fields
were analyzed with the use of a grid developed by Merz and Schenk (1970).
Knowing the area covered by the grid, it was possible to estimate the
volumetric density of bone and connective tissue and of the implanted materials
in the alveolus by counting the points on these structures (1000 per alveolus
analyzed, corresponding to 10 microscopic fields times 100 grid points).
The evaluation was made on the projection and drawing of the structures
on a 100-point grid printed on paper, with a final magnification of 1050X.
The volumetric density of bone and connective tissue in the alveolus was
estimated by the method of point counting.
Data were analyzed statistically by analysis of variance (ANOVA) and
by the Tukey test.
Results
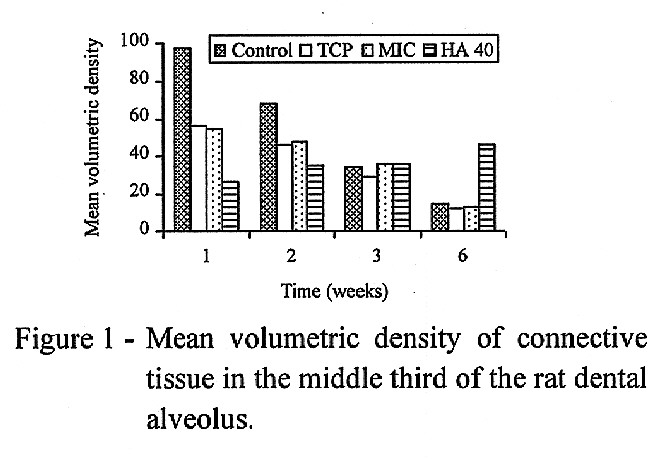
Figure 1 shows the mean percentages of the volumetric density of connective
tissue in the middle third of the rat dental alveolus evaluated 1, 2, 3
and 6 weeks after the implant. ANOVA showed a significant reduction in
the volumetric density of connective tissue along these periods of time
(F = 246.33; d.f. = 3; P<0.001). The control group presented a larger
amount of connective tissue than the other groups (F = 66.75; d.f. = 3;
P<0.001). A significant difference was also detected for time x treatment
interaction (F = 85.51; d.f. = 9; P<0.001). Tukey's test showed that
the control group presented higher volumetric density of the connective
tissue than the other groups at 1 and 2 weeks. At these times, the group
implanted with MIC was not different from the group implanted with TCP,
but both groups presented more connective tissue than the group implanted
with HA 40. After 6 weeks, the group implanted with HA 40 showed higher
volumetric density of connective tissue than the other groups.
Figure
1 - Mean volumetric density of connective tissue in the middle third of
the rat dental alveolus.
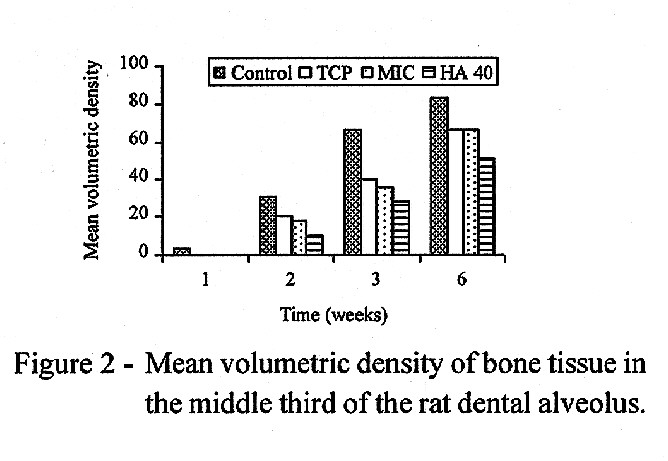
Figure 2 shows the mean percentages of volumetric density of bone tissue,
evaluated in the middle third of the rat dental alveolus 1, 2, 3 and 6
weeks after the implant. ANOVA showed a significant increase in the volumetric
density of bone tissue along the observation periods (F = 1008.23; d.f.
= 3; P<0.001). A significant difference was also detected between treatments
(F = 109.23; d.f. = 3; P<0.001). The Tukey test showed a higher volumetric
density in the control than in the other groups, as well as a higher density
in the groups implanted with MIC and TCP than in the group implanted with
HA 40. A significant difference was found for time x treatment interaction
(F = 13.19; d.f. = 9; P<0.001). Tukey's test showed no difference between
groups one week after the implant, but 2, 3, and 6 weeks after there was
a higher volumetric density of bone in the control than in the other groups.
No difference was detected between groups implanted with MIC and TCP during
these periods, but both groups showed a higher bone volume than the group
implanted with HA 40 3 and 6 weeks after the implant.
Figure
2 - Mean volumetric density of bone tissue in the middle third of the rat
dental alveolus.
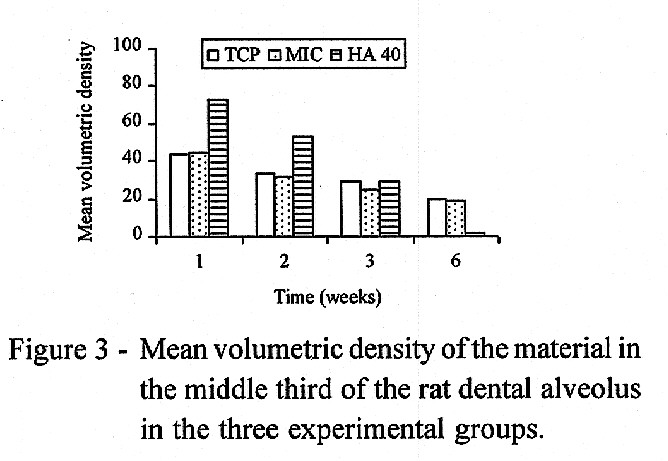
Figure 3 shows the mean percentages of volumetric density of the implanted
material, evaluated in the middle third of the rat dental alveolus 1, 2,
3 and 6 weeks after the implant. ANOVA showed a significant reduction of
the implanted materials along the observation periods (F = 35.73; d.f.
= 3; P<0.001). The group implanted with HA 40 presented a larger amount
of material than the other groups (F = 22.86; d.f. = 2; P<0.001). A
significant difference was found for time x treatment interaction (F =
40.47; d.f. = 6; P<0.001). One and 2 weeks after the implant, the group
implanted with HA 40 presented higher volumetric density than the other
groups. After 3 weeks there was no difference between groups and after
6 weeks the group implanted with HA 40 showed a smaller volume of material
than the other groups.
Figure
3 - Mean volumetric density of the material in the middle third of the
rat dental alveolus in the three experimental groups.
Discussion
In the present study, analysis of the results for the groups that received
MIC, TCP and HA 40 implants showed that these materials caused qualitative
and/or quantitative alterations during the different phases of the process
of alveolar repair. All materials caused a delay in the repair process
and presented a distinct biological behavior. MIC and TCP showed a higher
compatibility with the repair tissues than HA 40. During the first week,
the amount of inflammatory infiltrate was similar in all groups. However,
in the control group and in the groups implanted with MIC and TCP the inflammation
decreased during the second week and disappeared during the third, while
in the group implanted with HA 40 an inflammatory response was observed
up to the third week.
The delay we observed in the repair is in accordance with the data reported
in a series of studies recently reviewed by Carvalho and Okamoto (1987)
in which the same findings were obtained after the intraalveolar implant
of different materials such as root canal sealers, "synthetic bone", polyurethane,
boplant, gelatin sponge, proplast, dentin and enamel fragments, and propolis.
In general, placing any material inside the dental alveoli retards to some
extent the repair process. This happens because the intraalveolar implants
disturb clot organization and injure the remaining periodontal ligament
(Carvalho and Okamoto, 1978). Implanting MIC, TCP and HA 40 into the alveoli
resulted in the formation of a smaller amount of connective tissue during
the initial phases (1 and 2 weeks) because these materials were occupying
the space that would be initially filled by the clot.
During the periods of study we observed that in the alveoli implanted
with MIC and TCP the amount of connective tissue and implanted material
decreased with increasing amount of bone tissue. From the second to the
third week a two fold increase in the amount of bone was noted and during
this period the decrease in the amount of connective tissue was more marked
than the decrease of the implanted materials. Thus, the materials were
incorporated into the formed bone, as confirmed by the histological aspect
of the trabecular bone surrounding MIC and TCP particles, with no foreign
body reaction and without any intense inflammatory infiltrate.
An increase in the amount of connective tissue was detected in the alveoli
implanted with HA 40 during the first three weeks, followed by a period
of stabilization. The implanted material was present in large amounts at
the beginning and decreased progressively up to the sixth week, when it
virtually disappeared from the middle third of the alveoli. The bone tissue
increased along the six week period of the study, but the final amount
was much smaller than in the other implanted or control groups. Although
it was possible to observe trabecular bone in contact with HA 40, no particle
completely surrounded by trabeculae was found. Furthermore, the amounts
of connective and bone tissues observed after six weeks, as well as the
absence of HA 40 in the middle third, indicate that the material is expelled
from the alveolus before repair can begin. This fact was confirmed by the
histological finding of large amounts of HA 40 in the cervical third. Even
after 6 weeks the cervical third of the alveoli was open, i.e., filled
only with material and connective tissue in maturation. When the animals
were sacrificed, it was possible to find fragments of the material that
projected outward from the alveoli.
Although the same method for alveolar filling was employed, different
amounts of material were detected in the alveoli during the first week,
a fact that interfered directly with the amount of connective tissue formed.
The groups implanted with MIC and TCP presented less material than the
group implanted with HA 40 and this may be a consequence of the differences
in the properties of the materials. Although it was implanted in the particulate
form, HA 40 appeared after one week as a compact block of material, which
hampered the growth of connective tissue between the particles. Physicochemical
analysis of this material showed that each particle of HA 40 is formed
by aggregated smaller particles that are covered with some type of agglutinant
(Granjeiro et al., 1992), and it is possible that, when immersed in biological
fluids, they join to form a block.
This difference between materials may also be responsible, at least
in part, for the differences in biological behavior. As both MIC and TCP
remain in particulate form, they may be more rapidly stabilized by the
infiltration of connective tissue between the particles, and this seems
to contribute to a reduction in the intensity of the inflammatory reaction
evoked by the materials and, consequently, to better compatibility (Jarcho
et al., 1977).
As to HA 40, it is possible that it did not reach an initial stabilization
because it became a block inside the alveoli, and the growth of connective
tissue may have led to exposure of the implants, with their consequent
expulsion from the alveoli. Such facts have been considered to be the cause
of the failure of hydroxylapatite implanted as blocks (Cranin et al., 1988).
Furthermore, it has been demonstrated that HA 40 has contaminants such
as titanium, strontium, iron, sulfur and potassium (Granjeiro et al., 1992),
and this must have contributed to the expulsion of the material from the
alveoli and to the presence of a longer-lasting inflammatory infiltrate
than in the other implanted groups.
In the initial phases from implantation up to the third week, the main
mechanism responsible for the disappearance of MIC and TCP must have been
the extrusion of particles through alveolar openings. This has been frequently
reported in the initial periods when an intraalveolar hydroxylapatite implant
is used (Sherer et al., 1987; Cranin et al., 1988). However, during the
third week trabecular bone almost closing the alveolar openings was observed,
preventing the extrusion of more particles thereafter. Thus, it seems that
the disappearance of materials between the third and sixth weeks occurred
as a consequence of their biodegradation. Considering that the stereological
analysis permitted the quantification of the materials, it was possible
to verify that the volumetric density of MIC changed from 25.64 to 10.98
and the volumetric density of TCP changed from 29.22 to 20.96. It was then
possible to estimate the absorption rates of MIC and TCP that were 26%
and 28%, respectively, during a 3 week period. This high absorption rate
of MIC is quite different from those of other hydroxylapatites that generally
are nonabsorbable materials (Jarcho, 1981).
Of the two mechanisms involved in the biodegradation of these materials,
chemical dissolution and phagocytosis (Jarcho, 1981), it seems that the
former was the main factor responsible for MIC and TCP absorption during
the period from 3 to 6 weeks. The amount of phagocytic cells observed from
3 to 6 weeks near these materials was too small to explain such a rapid
absorption by means of phagocytosis. The presence of a small number of
these cells could be due to the fact that both MIC and TCP are dense materials,
thus presenting a smoother surface. This hypothesis is supported by the
results of Gomi et al. (1993) who demonstrated that the rougher the surface
of hydroxylapatites and tricalcium phosphate, which occurs when these materials
are porous, the higher is the number of multinucleated giant cells in contact
with these surfaces. This occurs because the roughness of the surface has
a positive influence on the fusion of mononuclear precursors.
This process of chemical dissolution that these materials seem to present
is important because it may result in an increase of the amount of phosphate
and calcium ions in the medium. These ions, in turn, may be absorbed by
the cells, mainly by means of endocytosis, leading to an increase in the
mitogenic activity of the fibroblasts (Cheung and McCarty, 1985) and stimulating
RNA transcription and protein synthesis in osteoblasts (Gregoire et al.,
1990), thus contributing to the high compatibility of the materials.
Bonachela et al. (1992) suggested the use of MIC for alveolar filling
immediately after extraction, in order to keep the height and contour of
the alveolar ridge. This happens either because the implants prevent the
collapse of the bone walls (Denissen et al., 1989) or because they occupy
the place where bone should be (Block and Kent, 1986). Thus, when hydroxylapatites
are used with this objective it is desirable that the material act as a
permanent implant; considering its high absorption rate, this seems not
to occur with MIC.
Since both MIC and TCP are absorbable materials, they should be used
in those situations in which a temporary filling material is desired, which
is initially incorporated into the tissue and later replaced by it. Thus,
it would be of interest to investigate clinically the validity of employing
these materials in situations such as those of periodontal or surgical
bone defects.
References
Block MS, Kent JN: A comparison of particulate and solid root forms of
hydroxylapatite in dog extraction sites. J Oral Maxillofac Surg 44: 89-93,
1986
Bonachela WC, Molo Jr FA, Taga EM, Granjeiro JM: Manutenção
do rebordo alveolar com hidroxiapatita microgranular. Rev Gaúcha
Odont 40: 212-213, 1992
Carvalho ACP, Okamoto T: Implantes intra-alveolares: considerações
sobre estudos experimentais. Rev Assoc Paul Cirurg Dent 32: 273-279, 1978
Carvalho ACP, Okamoto T: Reparação do alvéolo dental.
In: Cirurgia bucal: fundamentos experimentais aplicados à clínica.
55-80, Panamericana, São Paulo, 1987
Cheung HS & McCarty DJ: Mitogenesis induced by calcium containing
crystals: role of intracellular dissolution. Exp Cell Res 157: 63-70, 1985
Cranin AN, Ronen E, Shpuntoff R, Tobin G, Dibling JB: Hydroxylapatite
particulate versus cones as post-extraction implants in humans. J Biomed
Mater Res 22: 1165-1180, 1988
De Wijs FLJA, De Putter C, De Lange GL, De Groot K: Local residual augmentation
with solid hydroxylapatite blocks: Part II - correction of local resorption
defects in 50 patients. J Prosthet Dent 69: 510-513, 1993
Denissen HW, Kalk W, Veldhuis AAH, Hoof A: Eleven year study of hydroxylapatite
implants. J Prosthet Dent 61: 706-712, 1989 Gomi K, Lowenberg B, Shapiro
G, Davies JE: Resorption of sintered synthetic hydroxylapatite by osteoclasts
in vitro. Biomaterials 14: 91-96, 1993
Granjeiro JM, Taga EM, Fonseca M, Maeda L, Taga MSL, Trebachetti CR,
Negrato MLAB: Hidroxiapatita para uso clínico: caracterização
físico-química. Rev Gaúcha Odont 40: 130-134, 1992
Gregoire M, Orly I, Menateau J: The influence of calcium phosphate biomaterials
on human bone cell activities. J Biomed Mater Res 24: 165-177, 1990
Jarcho M, Kay JF, Gumaer KI, Doremus RH, Drobeck HP: Tissue, cellular
and subcellular events at a bone-ceramic hydroxylapatite interface. J Bioeng
1: 79-92, 1977
Jarcho M: Calcium phophate ceramics as hard tissue prosthetics. Clin
Orthop 157: 259-278, 1981
Merz WA, Schenk RK: Quantitative structural analysis of human cancellous
bone. Acta Anat 75: 54-66, 1970
Sherer AD, Slighter RG, Rothstein SS, Drobeck HP: Evaluation of implant
Durapatite particles in fresh extraction sockets to maintain the alveolar
ridge in beagle dogs. J Prosthet Dent 57: 331-337, 1987
Correspondence: Adalberto Luiz Rosa, Departamento de Cirurgia,
Faculdade de Odontologia de Ribeirão Preto, USP, Av. do Café
s/n, 14040-904 Ribeirão Preto, SP, Brasil.
|







{kind=link}
{kind=link}
{kind=link}