Iontophoresis: An Alternative in the Treatment of Incipient Caries?
José Leonardo SIMONE[1,2]
Flávio Eduardo Guillin PERES[1,2]
Mauricio Rufaiel MATSON[2]
Flávio F. de Godoy PERES[3]
Marcelo Munhões ROMANO[1]
[1]Disciplina de Clínica Integrada, Departamento de Estomatologia,
Faculdade de Odontologia, Universidade de São Paulo
[2]Disciplina de Clínica Integrada, Departamento de Ciências
da Saúde, Universidade Paulista, UNIP
[3]Cirurgião Dentista São Paulo, SP, Brasil
Braz Dent J (1995) 6(2): 123-129 ISSN 0103-6440
| Introduction | Material/Methods
| Discussion
| References
|
This study deals with some aspects of caries decay etiology and treatment
using iontophoresis, when there is no cavity, and discusses remineralization
of decayed teeth.
Key words:iontophoresis, fluoride, remineralization.
Introduction
Dental decay is caused by acids produced by microbial enzymatic action
on ingested carbohydrate. Fluoride, oral hygiene and saliva interfere in
this process. These acids decalcify the inorganic portion of the tooth,
the organic portion is then disintegrated, creating cavities. However,
this process can be reverted as long as the superficial layer of the tooth
remains intact.
Several authors have studied the phenomenon of remineralization through
deposition of calcium fluoride using different methods, such as topical
or systemic fluoride and the iontophoresis apparatus. The scientific basis
is that when fluoride ions are introduced in the lesion, they induce the
precipitation of calcium and phosphate on the crystals which are partially
demineralized.
Keys (1969) was the first to define caries decay etiology when he stated
that dental caries are the result of the interaction of three essential
factors: bacterial colonization of the surface of the tooth, called bacterial
plaque, fermented carbohydrates and the host tissue.
The interaction between bacterial plaque and fermented carbohydrates,
mainly sucrose, produces organic acids which reduce the pH of the plaque.
When the pH level drops to low levels such as 5.0 or 5.5 (critical pH)
, there is a dissolution of the crystals of the hydroxylapatite of the
enamel, resulting in a loss of mineral substances.
Bacterial plaque is formed by bacterial adherence to the acquired enamel
pellicle (AEP). Specific mechanisms of adherence allow some bacteria to
adhere even to smooth surfaces, causing the development of dental decay
on such surfaces (Loesche, 1986). Streptococcus mutans, for example, has
its own mechanism of adherence, revealed by the production of a polysaccharide
matrix called glucan (Loesche, 1986). Glucan is produced by the release
of glycosyltransferase (GTF) molecules, which adsorb to the acquired enamel
pellicle. The adsorbed GTF molecules can produce glucans when exposed to
sucrose. The volume of the produced matrix will enhance acid concentration
on the enamel-plaque interface. The acid conditions of the plaque and the
presence of fermentable dietary substracts lead to a degree of demineralization
that will result in subsurface lesions of the enamel, known as incipient
caries, clinically identified as a white opaque spot. Microscopy investigations
have shown that the layer covering an enamel lesion is a mineral-rich area,
whereas the subsurface area is low in mineral, though both are porous areas.
Silverstone et al. (1988) showed that small lesions of enamel caries beneath
a well mineralized surface layer consisted of four histological zones:
the dark zone and the surface zone, that are formed as a result of remineralization
phenomena, and the translucent zone and the body of the lesion, which are
produced as a result of demineralization. Experiments showed that these
lesions are able to remineralize as long as there is an intact surface
(Larsen and Fejerskov, 1987).
Since the Industrial Revolution and the consequent high amount of sugar
production, the number of dental decays has risen tremendously. However,
significant reduction in the prevalence of dental caries has been observed
over the past decades in some developed countries, owing to many factors,
among them, the use of topical fluorides. This has not been observed in
developing countries.
According to Eriksen and Bjertness (1991), there are a number of secondary
factors that may elucidate an additional dimension of the multifactorial
etiology of dental caries, such as fluoride, saliva buffer capacity, oral
hygiene, etc. Silverstone and Poole (1968) verified that after exposure
to either saliva or the calcifying solution, both natural and artificial
lesions showed histological remineralization. After four weeks, the authors
observed with a polarizing microscope and microradiographs that not only
had the dark zone surrounding the carious lesion appeared much broader,
but there was also a significant reduction of porosity at the surface,
proving that saliva has an important role on the remineralization process.
The reduction of caries through water fluoridation is not only due to systemic
effects, but also to its topic effects in the remineralization process.
Von der Fehr et al. (1970) showed that topical applications of fluoride
and good oral hygiene cause remineralization of incipient caries lesions.
This study demonstrated that incipient, smooth surface caries can be produced
experimentally in the course of 23 days, when active oral hygiene procedures
are abolished and frequent sucrose rinses are performed. After sixty days
of meticulous oral hygiene and daily mouthrinses with 0.2% NaF there was
regression of enamel lesions. Moreover, topical fluoride application reduced
demineralization.
Meyerowitz et al. (1991) studied the effect of a twice daily topical
application of a 0.05 % NaF mouthrinse in the oral cavities of subjects
suffering from irradiation-induced hyposalivation, during a period of 28
days. The results suggest that this oral rinse can prevent demineralization
and enhance remineralization.
Even in the presence of low levels of fluoride in the solution phase,
crystallization of the lesion is enhanced, while the corresponding dissolution
is retarded. The remineralization rate appears to be proportional to the
degree of supersaturation of the solution containing calcium and phosphate
ions. The presence of enamel pellicles and salivary macromolecules actually
inhibits the formation of basic calcium phosphates which is enhanced by
fluoride at low concentrations (Ten Cate, 1990).
One of the prerequisites of the remineralization of the lesion is the
existence of partially demineralized crystals which work as centers of
mineral disposal. The formation of new crystals requires a much higher
concentration of calcium and phosphates than is usually found in the saliva
(Ten Cate, 1990).
Silverstone at al. (1988) quantified the effect that fluoride solutions
(1 ppm) had on the degree of remineralization of enamel lesions. Scanning
electron micrograph showed that these crystals have diameters greater than
those of sound enamel making it clear why remineralized lesions are more
resistant.
There is evidence that a major part of the fluoride that is retained
on teeth during topical application is calcium fluoride and calcium fluoride-like,
and that this material is relatively stable in the mouth. This is due to
surface absorption of phosphate ions onto the calcium fluoride surface.
Calcium fluoride releases fluoride during caries changes due to reduced
concentration of phosphate at acid pH. (Ogaard, 1990; Rolla and Saxegaard,
1990). The fluoride released during caries challenges may interact in demineralization
caused by the process of the plaque.
Gangarosa (1983) studied a new method of applying ionic drugs through
electrical currents into surface tissues in order to achieve a therapeutic
level. This method is called iontophoresis. According to Gangarosa (1983),
the ion movements in iontophoresis follow some physical laws, which must
be learned in order to make it able to control the operation. Ohm's Law
states that: V = I.R, that is electromotive force (V, in volts) equals
current (I, in amps) times resistence (R, in ohms). Therefore, the current
level, which quantifies the electron movement in an electric conductor
or electrolytic solution is directly proportional to electromotive force
and inversely proportional to electrical resistance. Coloumb's Law, a second
law which has usefulness for dental iontophoresis, states that: Q = I.T,
that is, the quantity of electricity (Q) delivered is obtained by multiplying
amperage (milliamps) times time (T, min). A third electrical law of importance
is Faraday's Law, which states the amount of fluoride ions delivered in
the incipient caries decay is directly proportional to the quantity of
energy (Q), which means, to time and current.
It was observed that when the concentration of fluoride in topical application
is high, there is an increase in the formation of calcium fluoride. (Saxegaard
and Rolla 1988; Rolla and Saxegaard, 1990).
According to Oggard (1990) calcium fluoride is formed during topically
applied fluoride, and can be released into the lesion, resulting in remineralization
and difficulty of dissolution.
Walton et al. (1979) studied the pulpal reaction towards an amount of
current applied to the teeth. They applied 1% sodium fluoride iontophoretically
on exposed roots of dogs and it was concluded that iontophoresis causes
no histological changes to pulpal tissues. Two current dosages were used:
a therapeutic dosage of 0.5 mA for 2 min (0.06 Coloumbs) and a high current
dosage of 1.0 mA for 5 min (0.3 Coloumbs). After 7 and 80 days, different
groups of teeth were extracted and histologically examined.
Material and Methods
Five patients, 6 to 12 years old, with two or more incipient caries were
treated with the following method. No plaque control orientation was given
either before or after treatment. Initially, a clinical examination and
O'Leary's index were made. This is a plaque index which is used to give
a notion of the patient's hygiene by the following formula using teeth
coloration: number of colored surfaces/number of surfaces X 100.
A total of 12 lesions were treated iontophoretically with a solution
of 500 ppm (NaF, 26.315 mM), enough for good remineralization according
to studies by Damato et al. (1990).
The iontophoresis machine was manufactured by the principles of Gangarosa
(1988), Parr and Brokaw (1989), and made by a variable source (0-24 volts,
constant current) supply for commercial energy (110 volts) (Figure 1).
Figure
1 - Iontophoresis machine.
The anode (the positively charged electrode) covered with gauze soaked
in physiological saline was held by the patient. The cathode (the negative
electrode) in the shape of a tubular bush filled with a 500 ppm NaF solution
was placed on the lesion, after absolute isolation and prophylaxis with
pumice-stone and water were done. A micro-amperimeter (YUFONG Digital multitester)
in line with the anode was used to control the intensity of the current
at 0.1 mA. The application lasted 2 min. These procedures were repeated
every week for about one month.
Evaluation Criteria: Clinical examinations and O'Leary's Index were
recorded before and after the procedures. The lesions were evaluated through
slides (Ektacrome 65, 35 mm), according to the technique of Edgard et al.
(1978) and the caries index of Von der Fehr et al. (1970).
The first pictures were taken after prophylaxis was done to start the
first application, and the last ones were taken 40 days later. The camera
(Yashica Dental) was used at a distance of about 10 cm so that the angle
between the axis of the lens and the tooth surface was approximately 60-70
degrees.
The Caries Index of Von der Fehr was used to evaluate the enamel surface:
0 - normal enamel; 1 - slight pearly-grey opacity; 2 - speckled greyish-yellow
area; 3 - diffuse white area; 4 - well-defined white-spot, shiny surface;
5 - chalky-white spot, loss of surface sheen.
Discussion
This study used a 0.1 mA intensity of current for 2 min (0.012 Coloumbs),
5 times smaller than the therapeutic dosage used by Walton et al.(1979).
This low intensity of current was used in order to avoid any damage of
the pulp, discomfort to the patient and, moreover, to prevent formation
of high quantities of calcium fluoride on the porous surface of the lesion.
This could inhibit a higher penetration of the free fluoride inside the
lesion and a deeper remineralization.
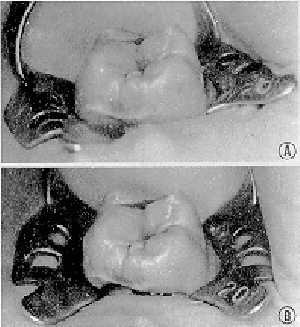
The active lesions of the incipient caries at level 5 (Figure 2, top)
were clinically reduced after 40 days to level 4 (Figure 2, bottom). During
this procedure, there was a high concentration of fluoride on the demineralized
surface due to the formation of calcium fluoride which was proportional
to its disponibility.
Figure
2 - Top, Lesions of the incipient caries at level 5. Bottom, Lesions
of the incipient caries clinically reduced to 1 at level 4 after 40 days.
Gelhard and Arend (1984) state that the remineralization rate is faster
during the first 2 weeks, so it cannot be expected that after 40 days the
lesions decreased to lower levels than they are.
Considering the data obtained from literature and clinical findings,
despite the small number of subjects, we can conclude that there was clear
evidence of remineralization in the cases studied.
This procedure is a rapid and inexpensive method; however, further studies
should be carried out in order to provide more scientific support.
References
Damato FA, Strang R, Jenkins GN: Effects of fluoride concentration on remineralization
of carious enamel: an in vitro pH-cycling study. Caries Res 24 :174 180,
1990
Edgard WM, Rug-Gunn AJ, Jenkins GN, Geddes DAM: Photographic and direct
visual recording of experimental caries like changes in human dental enamel.
Arch Oral Biol., 23: 667-673, 1978
Eriksen HM, Bjertness E: Concepts of health and diseases and caries
prediction: a literature review. Scand J Dent Res 99: 476-483,1991
Featherstone JDB, Glena R, Shadiati M, Shields CP: Dependence of in
vitro demineralization of apatite and remineralization of dental enamel
on fluoride concentration. J Dent Res 69 (Special Issue): 620-625, 1990
Gangarosa LP: Iontophoresis in dental practice. Chicago, Quintessence,
1983 Gangarosa LP: Electrical medication (Iontophoresis): a modality for
expanding dental practice with new therapies. Gen Dent 36: 402-403, 1988
Gelhard TBFM, Arends J: In vivo remineralization of artificial subsuperficial
lesions in human enamel. J Biol Buc-cale 12: 49-57, 1984
Keys PH: Present and future measures for dental caries control. J Amer
Dent Assoc 79: 1395-1404, 1969
Larsen MJ, Fejerskov O: Remineralization from a clinical point of view.
Dtsch Zahnarztl Z 42 (Suppl 1): 91-92, 1987
Loesche WJ: Role of Streptococcus mutans in human dental decay. Microbiol
Rev 50: 353-379, 1986
Meyerowitz C, Featherstone JDB, Billings RJ, Eisenberg AD, Fu J, Shariati
M, Zero AT: Use of an intra-oral model to evaluate 0.05% sodium fluoride
mouthrinse in radiation-induced hypo-salivation. J Dent Res 70: 894-898,
1991
Ogaard B: Effects of fluoride on caries development and progression
in vivo. J Dent Res 69 (Special Issue): 813-819, 1990
Parr Jr OD, Brokaw WC: Economical iontophoresis for dentistry. Quintessence
Int 20: 841-845, 1989
Rolla G, Saxegaard E: Critical evaluation and use of topical fluorides,
with emphasis on calcium fluoride in caries inhibition. J Dent Res 69 (Special
Issue) 780-785, 1990
Saxegaard E, Rolla G: Fluoride acquisition on and in human enamel during
topical application in vitro. Scand J Dent Res 96: 523-535, 1988
Silverstone LM, Poole DFG: The effect of saliva and calcifying solutions
upon the histological appearance of enamel. Caries Res 2: 87-96, 1968
Silverstone LM, Hicks MJ, Featherstone JDB: Dynamic factors affecting
lesion initiation and progression in human dental enamel. Part 1. The dynamic
nature of enamel caries. Quintessence Int 19: 693-710, 1988
Ten Cate JM: In vitro studies on the effects of fluoride on de and remineralization.
J Dent Res 69 (Special Issue): 614-619, 1990
Von der Fehr FR, Lõe H, Thieilade E: Experimental caries in man.
Caries Res 4: 131-148, 1970
Walton RE, Leonard LA, Sharawy M, Gangarosa LP: Effects on pulp and
dentin of iontophoresis of sodium fluoride on exposed roots in dogs. Oral
Surg. 48: 545-557, 1979
Correspondence:Prof. Dr. José Leonardo Simone, Av. Lineu
Prestes, 2227, Cidade Universitaria, Butantã 05508-900, São
Paulo, SP, Brasil.
|







{kind=link}
{kind=link}