Odontoma-Producing Intraosseous Calcifying Odontogenic Cyst: Case Report
Gustavo D. Pistóia1
Raquel F. GERLACH2
Júlio César B. dos Santos1
Agenor Montebelo Filho1
Departments of 1Oral Diagnostics and 2Morfology,Faculty
of Dentistry of Piracicaba, UNICAMP,Piracicaba, SP, Brazil
Correspondence: Dr. Agenor Montebelo Filho, Disciplina de Radiologia,
Faculdade de Odontologia de Piracicaba, UNICAMP, Av. Limeira, 901, 13414-900
Piracicaba, SP, Brasil. tel: +55-19-430-5327. Fax: +55-19-430-5218. e-mail:
montebel@fop.unicamp.br
Braz Dent J (2001) 12(1): 67-70
ISSN 0103-6440
INTRODUCTION | CASE
REPORT | DISCUSSION | RESUMO
| REFERENCES
The present report describes a case of odontoma-producing intraosseous
calcifying odontogenic cyst in a 36-year-old Black male in the right mandibular
bicuspid region. The lesion involved an unerupted permanent canine, which
was displaced to the mandible base and a calcified mass that was later
recognized as an odontoma. The lesion was surgically removed.
Key Words: odontogenic cyst, Gorlin cyst.
INTRODUCTION
Calcifying odontogenic cyst was first categorized as a distinct entity
by Gorlin et al. (1), and was named after him since then. According
to Shear (2), it accounts for 1% of jaw cysts. As the number
of reports increased, it was proposed that calcifying odontogenic cyst
was indeed a heterogeneous group of entities, with distinct histopathologic
findings. We present a case of intraosseous odontoma-producing calcifying
odontogenic cyst involving an unerupted permanent canine.
CASE REPORT
A 36-year-old Black male complained of a painless swelling in the right
bicuspid region of the mandible. Intraoral examination revealed a firm
enlargement in the buccal right bicuspid region extending from the canine
to the second bicuspid. The overlying mucosa had a normal aspect. The deciduous
right canine was still present, and the permanent one was missing. Detailed
examination of the involved teeth revealed no mobility or tenderness to
palpation. There were also no signs of caries, pulp pathosis or periodontitis.
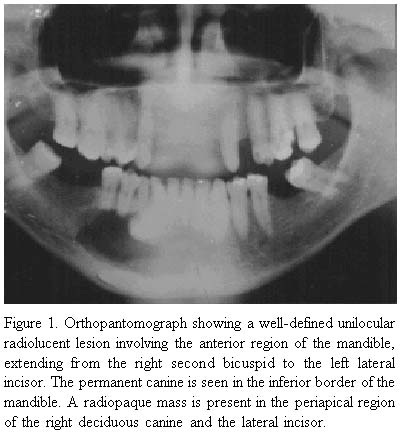
A panoramic radiograph (Figure 1) revealed
a well-defined unilocular radiolucent lesion involving the anterior region
of the mandible, extending from the right second bicuspid to the left lateral
incisor. The permanent canine was displaced to the inferior border of the
mandible. A radiopaque mass was present in the periapical region of the
right deciduous canine and the lateral incisor. The right bicuspids exhibited
marked root resorption. Radiological differential diagnosis included adenomatoid
odontogenic tumor, intraosseous calcifying odontogenic cyst, cystic odontoma,
ossifying fibroma, ameloblastic fibro-odontoma and calcifying epithelial
odontogenic tumor. Calcifying epithelial odontogenic tumor is most often
found in the posterior region of the mandible, and the margins of this
lesion are often scalloped(3). Ameloblastic fibro-odontoma is usually encountered
in children of 10 years of age, on average. Although ossifying fibroma
has many features in common with this case, it is seen more often in females.
As an additional step, aspiration was performed, and the fluid obtained
confirmed the cystic nature of the lesion.
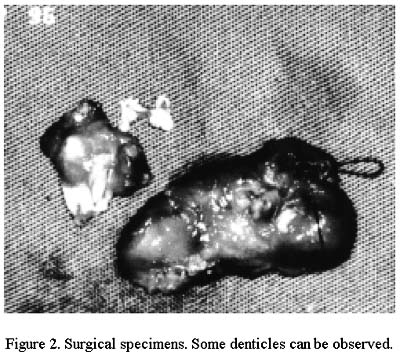
The teeth involved in the lesion received endodontic treatment before
the surgical excision of the lesion, during which the involved permanent
canine was also removed (Figure 2). Healing
proceeded uneventfully.
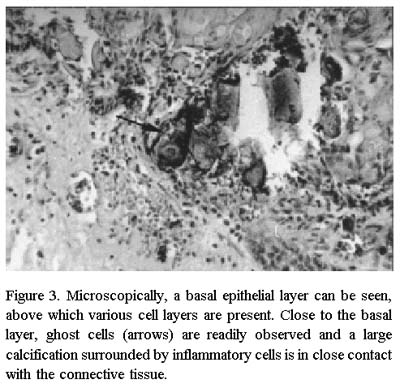
Microscopically, a cystic lesion was observed, which was lined with
a basal layer of columnar cells whose nuclei were located next to the basement
membrane (Figure 3). Above this layer, there
was a variable number of cell layers. In some places, loosely arranged
cells could be seen resembling stellate reticulum cells, and intermixed
with them, ghost cells and calcifications. Ghost cells have been regarded
as pathognomonic for calcifying odontogenic cyst for a long time, and are
recognized by their characteristic eosinophilic appearance. Denticles were
also present, leading to the diagnosis of odontoma-producing intraosseous
unicystic calcifying odontogenic cyst.
DISCUSSION
Since 1971, calcifying odontogenic cyst has been described by the World
Health Organization as a non-neoplastic cystic lesion in which the epithelial
lining shows a well-defined basal layer that is often many cells thick
and that may resemble the stellate reticulum of an enamel organ, and masses
of ghost epithelial cells that may be in the epithelial cyst lining or
in the fibrous capsule (4). The ghost cells may become calcified
and dysplastic dentin may be laid down next to the basal cell layer of
the epithelium. It may be associated with complex odontoma or with tissue
resembling an ameloblastic fibro-odontoma.
As the number of reports increased, it was proposed that calcifying
odontogenic cyst was indeed a heterogeneous group of entities, with distinct
histopathologic findings that included a solid tumor. Praetorius (5) proposed
a subclassification for the heterogeneous group of calcifying odontogenic
cysts, in which the cystic lesions were separated from the neoplasms (solid
lesions). These researchers further divided the cystic entity into three
types, the simple unicystic type, the unicystic odontoma-producing type,
and the ameloblastomatous proliferating type. Calcifying odontogenic cyst
may be otherwise described sa developmental odontogenic lesion that has
its cutaneous counterpart in Malherbe's calcifying epithelioma
(1,6).
This case report is in agreement with the literature finding that calcifying
odontogenic cysts occur predominantly as an intraosseous lesion. Other
authors have reported only 13 to 21 percent of the cysts to be peripheral
(extraosseous) lesions (7,8). The area affected in this case has been considered
the most commonly affected site: about 65% of the reported cases were found
in the incisor-canine area (3,7). The age of the patient is
also in agreement with the literature that the mean age when the calcifying
odontogenic cyst is diagnosed is 33 years (3). The radiographic findings
of this case (unilocular radiolucency with a radiopaque mass and well-circumscribed
borders) are encountered in the majority of odontoma-producing intraosseous
calcifying odontogenic cysts (9,10)
The radiopaque mass observed in the panoramic radiograph of this case,
later diagnosed as odontoma components, are considered to be present in
24-50% of the reported cases (3,7). These cases were classified
as a subtype of calcifying odontogenic cyst under the term odontoma-producing
type (7), or as a cystic variant associated with odontoma (4,8).
Hirschberg et al. (10) proposed that this variant should be classified
as a separate entity for which they suggested the name odontocalcifying
odontogenic cyst. They observed that this variant was more prevalent
in females, with a mean age at discovery of 16 years (compared with 34.4
years in the simple calcifying odontogenic cyst group) and that most cases
were located in the maxilla. The findings of our case are not in accordance
with the above mentioned observations. Hirschberg et al. (10) claimed that
the separation of this variant from the heterogeneous group of calcifying
odontogenic cyst could lead to a better understanding of its pathogenesis.
Although the majority of the cases of this variant indeed have the features
pointed out by Hirschberg et al. (10), it may be noteworthy that these
characteristics may not be sufficient to classify this variant as a separate
entity. In this regard, our case may indicate that this variant may be
more common in younger adults, but it may also be discovered in older persons,
so that a different pathogenesis might not be associated with this variant.
The possibility of occur rence of an odontoma associated with calcifying
odontogenic cyst may result from factors present at a certain age, but
it seems that the same odontogenic epithelium is present in calcifying
odontogenic cyst and in this particular variant. Furthermore, it seems
that the same characteristic epithelium is involved in the various clinical
presentations of this lesion.
In spite of the low frequency of this lesion and the fact that most
cases are surgically removed and heal uneventfully, there must be a close
follow-up, because there have been reports of association with carcinoma,
adenomatoid tumor and ameloblastoma (11-13).
ACKNOWLEDGMENTS
G.D. Pistóia was supported with a Master's fellowship (PICDT)
from CAPES.
RESUMO
Pistóia GD, Gerlach RF, dos Santos JCB, Montebelo Filho A. Odontoma
produzindo cisto odontogênico calcificante intra-ósseo: relato
de caso. Braz Dent J 2001;12(1):67-70.
O presente relato descreve um caso de odontoma que produziu um cisto
odontogênico calcificante, num homem de 36 anos, da raça negra,
na região de premolares inferiores direitos. A lesão envolveu
um canino permanente não irrompido, o qual foi deslocado para a
base da mandíbula e uma massa calcificada que foi posteriormente
reconhecida como um odontoma. A lesão foi removida cirurgicamente.
Unitermos: cisto odontogênico, cisto de Gorlin.
REFERENCES
1. Gorlin RJ, Pindborg JJ, Clausen F, Vickers, RA. The calcifying odontogenic
cyst _ a possible analogue of the cutaneous calcifying epithelioma of Malherbe.
Oral Surg Oral Med Oral Pathol 1962;15:1235-1243.
2. Shear M. Developmental odontogenic cysts. An update. J Oral Pathol
Med 1994;23:1-11.
3. Waldron CA. Odontogenic cysts and tumors. In: Oral & Maxillofacial
Pathology. Neville BW, Damm DD, Allen CM, Bouquot JE. eds. 1st edn. Philadelphia:
Saunders, 1995. pp 493-538.
4. Pindborg JJ, Kramer IRH, Torloni H. Histological typing of odontogenic
tumors, jaw cysts, and allied lesions. Geneva: World Health Organization,
1971. pp 28-35.
5. Praetorius F, Hjorting-Hansen E, Gorlin RJ, Vickers RA. Calcifying
odontogenic cyst: Range, variations and neoplastic potential. Acta Odontol
Scan 1981:39:227-240.
6. Lever WG, Schaumberg-Lever G. Histopatologia da pele (translated
by Nelson Gomes de Oliveira from: Histopathology of the skin - 7th
edition). São Paulo: Manole, 1991.
7. Buchner A. The central (intraosseous) calcifying odontogenic cyst:
an analysis of 215 cases. J Oral Maxillofac Surg 1991;49:330-339.
8. Johnson A, Fletcher M, Gold L, Chen S-Y. Calcifying odontogenic cyst:
A clinicopathologic study of 57 cases with immunohistochemical evaluation
for cytokeratin. J Oral Maxillofac Surg 1997;55:679-683.
9. Hong SP, Ellis GL, Hartman KS. Calcifying odontogenic cyst. Oral
Surg Oral Med Oral Pathol 1991;72:56-64.
10. Hirshberg A, Kaplan I, Buchner A. Calcifying odontogenic
cyst associated with odontoma: a possible separate entity (odontocalcifying
odontogenic cyst). J Oral Maxillofac Surg
1994;52:555-558.
11. Tajima Y, Yokose S, Sakamoto E, Yamamoto Y, Utsumi N. Ameloblastoma
arising in calcifying odontogenic cyst. Oral Surg Oral Med Oral Pathol
1992;74:776-779.
12. Tanaka N, Iwaki H, Yamada T, Amagasa T. Carcinoma after enucleation
of a calcifying odontogenic cyst. J Oral Maxillofac Surg 1993;51:75-78.
13. Zeitoun IM, Dhanrajani PJ, Mosadomi HA. Adenomatoid odontogenic
tumor arising in a calcifying odontogenic cyst. J Oral Maxillofac Surg
1996;54:634-637.
|







{kind=link}
{kind=link}
{kind=link}